What should be my HDL cholesterol?
HDL cholesterol levels are a rough measure of HDL particle quantity in the blood. They actually tell us next to nothing about HDL particle type, although HDL cholesterol increases are usually associated with increases in LDL particle size. This a good thing, since small-dense LDL particles are associated with increased cardiovascular disease.
Most blood lipid panels reviewed by family doctors with patients give information about HDL status through measures of HDL cholesterol, provided in one of the standard units (e.g., mg/dl).
Study after study shows that HDL cholesterol levels, although imprecise, are a much better predictor of cardiovascular disease than LDL or total cholesterol levels. How high should be one’s HDL cholesterol? The answer to this question is somewhat dependent on each individual’s health profile, but most data suggest that a level greater than 60 mg/dl (1.55 mmol/l) is close to optimal for most people.
The figure below (from Eckardstein, 2008; full reference at the end of this post) plots incidence of coronary events in men (on the vertical axis), over a period of 10 years, against HDL cholesterol levels (on the horizontal axis). Note: IFG = impaired fasting glucose. This relationship is similar for women, particularly post-menopausal women. Pre-menopausal women usually have higher HDL cholesterol levels than men, and a low incidence of coronary events.

From the figure above, one can say that a diabetic man with about 55 mg/dl of HDL cholesterol will have approximately the same chance, on average, of having a coronary event (a heart attack) as a man with no risk factors and about 20 mg/dl of HDL cholesterol. That chance will be about 7 percent. With 20 mg/dl of HDL cholesterol, the chance of a diabetic man having a coronary event would approach 50 percent.
We can also conclude from the figure above that a man with no risk factors will have a 5 percent chance of having a coronary event if his HDL cholesterol is about 25 mg/dl; and about 2 percent if his HDL cholesterol is greater than 60 mg/dl. This a 60 percent reduction in risk, a risk that was low to start with because of the absence of risk factors.
HDL cholesterol levels greater than 60 are associated with significantly reduced risks of coronary events, particularly for those with diabetes (the graph does not take diabetes type into consideration). Much higher levels of HDL cholesterol (beyond 60) do not seem to be associated with much lower risk of coronary events.
Conversely, a very low HDL cholesterol level (below 25) is a major risk factor when other risk factors are also present, particularly: diabetes, hypertension (high blood pressure), and familial hypercholesteromia (gene-induced very elevated LDL cholesterol).
It is not yet clear whether HDL cholesterol is a cause of reduced cardiovascular disease, or just a marker of other health factors that lead to reduced risk for cardiovascular disease. Much of the empirical evidence suggests a causal relationship, and if this is the case then it may be a good idea to try to increase HDL levels. Even if HDL cholesterol is just a marker, the same strategy that increases it may also have a positive impact on the real causative factor of which HDL cholesterol is a marker.
What can one do to increase his or her HDL cholesterol? One way is to replace refined carbs and sugars with saturated fat and cholesterol in one’s diet. (I know that this sounds counterintuitive, but seems to work.) Another is to increase one’s vitamin D status, through sun exposure or supplementation.
Other therapeutic interventions can also be used to increase HDL; some more natural than others. The figure below (also from Eckardstein, 2008) shows the maximum effects of several therapeutic interventions to increase HDL cholesterol.
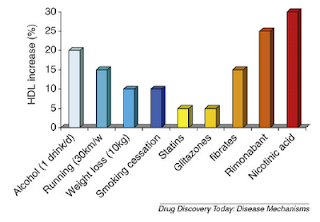
Among the therapeutic interventions shown in the figure above, taking nicotinic acid (niacin) in pharmacological doses, of 1 to 3 g per day (higher dosages may be toxic), is by far the most effective way of increasing one’s HDL cholesterol. Only the niacin that causes flush is effective in this respect. No-flush niacin preparations may have some anti-inflammatory effects, but do not cause increases in HDL cholesterol.
Rimonabant, which is second to niacin in its effect on HDL cholesterol, is an appetite suppressor that has been associated with serious side effects and, to be best of my knowledge, has been largely banned from use in pharmaceutical drugs.
Third in terms of effectiveness, among the factors shown in the figure, is moderate alcohol consumption. Running about 19 miles per week (2.7 miles per day) and taking fibrates are tied in forth place.
Many people think that they are having a major allergic reaction, and have a panic attack, when they experience the niacin flush. This usually happens several minutes after taking niacin, and depends on the dose and whether niacin was consumed with food or not. It is not uncommon for one’s entire torso to turn hot red, as though the person had had major sunburn. This reaction is harmless, and usually disappears after several minutes.
One could say that, with niacin: no “pain” (i.e., flush), no gain.
Reference:
von Eckardstein, A. (2008). HDL – a difficult friend. Drug Discovery Today: Disease Mechanisms, 5(3), 315-324.
Most blood lipid panels reviewed by family doctors with patients give information about HDL status through measures of HDL cholesterol, provided in one of the standard units (e.g., mg/dl).
Study after study shows that HDL cholesterol levels, although imprecise, are a much better predictor of cardiovascular disease than LDL or total cholesterol levels. How high should be one’s HDL cholesterol? The answer to this question is somewhat dependent on each individual’s health profile, but most data suggest that a level greater than 60 mg/dl (1.55 mmol/l) is close to optimal for most people.
The figure below (from Eckardstein, 2008; full reference at the end of this post) plots incidence of coronary events in men (on the vertical axis), over a period of 10 years, against HDL cholesterol levels (on the horizontal axis). Note: IFG = impaired fasting glucose. This relationship is similar for women, particularly post-menopausal women. Pre-menopausal women usually have higher HDL cholesterol levels than men, and a low incidence of coronary events.

From the figure above, one can say that a diabetic man with about 55 mg/dl of HDL cholesterol will have approximately the same chance, on average, of having a coronary event (a heart attack) as a man with no risk factors and about 20 mg/dl of HDL cholesterol. That chance will be about 7 percent. With 20 mg/dl of HDL cholesterol, the chance of a diabetic man having a coronary event would approach 50 percent.
We can also conclude from the figure above that a man with no risk factors will have a 5 percent chance of having a coronary event if his HDL cholesterol is about 25 mg/dl; and about 2 percent if his HDL cholesterol is greater than 60 mg/dl. This a 60 percent reduction in risk, a risk that was low to start with because of the absence of risk factors.
HDL cholesterol levels greater than 60 are associated with significantly reduced risks of coronary events, particularly for those with diabetes (the graph does not take diabetes type into consideration). Much higher levels of HDL cholesterol (beyond 60) do not seem to be associated with much lower risk of coronary events.
Conversely, a very low HDL cholesterol level (below 25) is a major risk factor when other risk factors are also present, particularly: diabetes, hypertension (high blood pressure), and familial hypercholesteromia (gene-induced very elevated LDL cholesterol).
It is not yet clear whether HDL cholesterol is a cause of reduced cardiovascular disease, or just a marker of other health factors that lead to reduced risk for cardiovascular disease. Much of the empirical evidence suggests a causal relationship, and if this is the case then it may be a good idea to try to increase HDL levels. Even if HDL cholesterol is just a marker, the same strategy that increases it may also have a positive impact on the real causative factor of which HDL cholesterol is a marker.
What can one do to increase his or her HDL cholesterol? One way is to replace refined carbs and sugars with saturated fat and cholesterol in one’s diet. (I know that this sounds counterintuitive, but seems to work.) Another is to increase one’s vitamin D status, through sun exposure or supplementation.
Other therapeutic interventions can also be used to increase HDL; some more natural than others. The figure below (also from Eckardstein, 2008) shows the maximum effects of several therapeutic interventions to increase HDL cholesterol.

Among the therapeutic interventions shown in the figure above, taking nicotinic acid (niacin) in pharmacological doses, of 1 to 3 g per day (higher dosages may be toxic), is by far the most effective way of increasing one’s HDL cholesterol. Only the niacin that causes flush is effective in this respect. No-flush niacin preparations may have some anti-inflammatory effects, but do not cause increases in HDL cholesterol.
Rimonabant, which is second to niacin in its effect on HDL cholesterol, is an appetite suppressor that has been associated with serious side effects and, to be best of my knowledge, has been largely banned from use in pharmaceutical drugs.
Third in terms of effectiveness, among the factors shown in the figure, is moderate alcohol consumption. Running about 19 miles per week (2.7 miles per day) and taking fibrates are tied in forth place.
Many people think that they are having a major allergic reaction, and have a panic attack, when they experience the niacin flush. This usually happens several minutes after taking niacin, and depends on the dose and whether niacin was consumed with food or not. It is not uncommon for one’s entire torso to turn hot red, as though the person had had major sunburn. This reaction is harmless, and usually disappears after several minutes.
One could say that, with niacin: no “pain” (i.e., flush), no gain.
Reference:
von Eckardstein, A. (2008). HDL – a difficult friend. Drug Discovery Today: Disease Mechanisms, 5(3), 315-324.