Being glucose intolerant may make you live only to be 96, if you would otherwise live to be 100
This comes also from the widely cited Brunner and colleagues study, published in Diabetes Care in 2006. They defined a person as glucose intolerant if he or she had a blood glucose level of 5.3-11 mmol/l after a 2-h post–50-g oral glucose tolerance test. For those using the other measurement system, like us here in the USA, that is a blood glucose level of approximately 95-198 mg/dl.
Quite a range, eh!? This covers the high end of normoglycemia, as well as pre- to full-blown type 2 diabetes.
In this investigation, called the Whitehall Study, 18,403 nonindustrial London-based male civil servants aged 40 to 64 years were examined between September 1967 and January 1970. These folks were then followed for over 30 years, based on the National Health Service Central Registry; essentially to find out whether they had died, and of what. During this period, there were 11,426 deaths from all causes; with 5,497 due to cardiovascular disease (48.1%) and 3,240 due to cancer (28.4%).
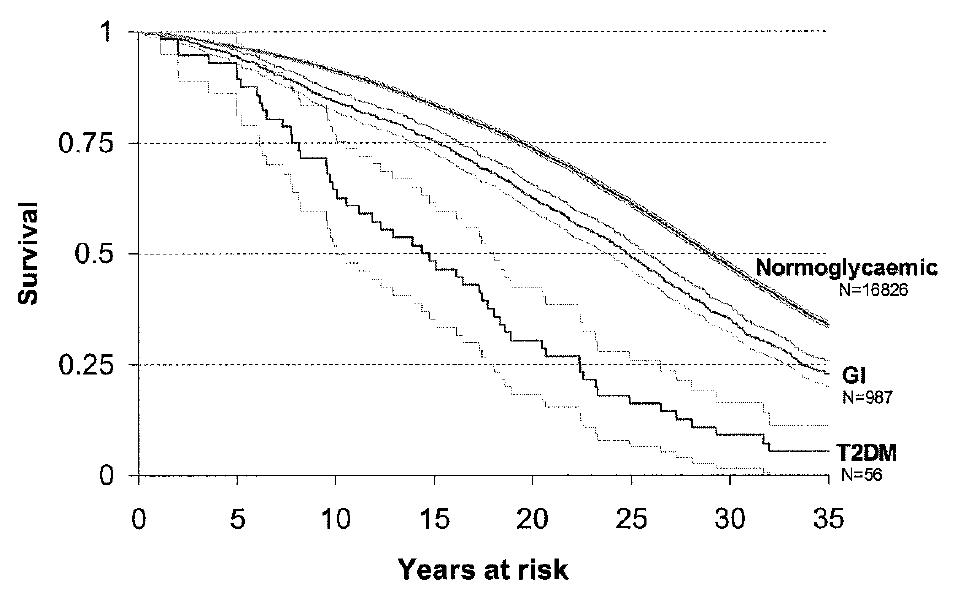
The graph below shows the age-adjusted survival rates against time after diagnosis. Presumably the N values refer to the individuals in the glucose intolerant (GI) and type 2 diabetic (T2DM) groups that were alive at the end of the monitoring period. This does not apply to the normoglycemic N value; this value seems to refer to the number of normoglycemic folks alive after the divergence point (5-10 years from diagnosis).

Note by the authors: “Survival by baseline glucose tolerance status diverged after 5-10 years of follow-up. Median survival differed by 4 years between the normoglycemic and glucose intolerant groups and was 10 years less in the diabetic compared with the glucose intolerant group.”
That is, it took between 5 and 10 years of high blood glucose levels for any effect on mortality to be noticed. One would expect at least some of the diagnosed folks to have done something about their blood glucose levels; a confounder that was not properly controlled for in this study, as far as I can tell. The glucose intolerant folks ended up living 4 years less than the normoglycemics, and 10 years more than the diabetics.
One implication of this article is that perhaps you should not worry too much if you experience a temporary increase in blood glucose levels due to compensatory adaptation to healthy changes in diet and lifestyle, such as elevated growth hormone levels. It seems unlikely that such temporary increase in blood glucose levels, even if lasting as much as 1 year, will lead to permanent damage to cells involved in glucose metabolism like the beta cells in the pancreas.
Another implication is that being diagnosed as pre-diabetic or diabetic is not a death sentence, as some people seem to take such diagnoses at first. Many of the folks in this study who decided to do something about their health following an adverse diagnosis probably followed the traditional advice for the treatment of pre-diabetes and diabetes, which likely made their health worse. (See Jeff O’Connell’s book Sugar Nation for a detailed discussion of what that advice entails.) And still, not everyone progressed from pre-diabetes to full-blow diabetes. Probably fewer refined foods available helped, but this does not fully explain the lack of progression to full-blow diabetes.
It is important to note that this study was conducted in the late 1960s. Biosynthetic insulin was developed in the 1970s using recombinant DNA techniques, and was thus largely unavailable to the participants of this study. Other treatment options were also largely unavailable. Arguably the most influential book on low carbohydrate dieting, by Dr. Atkins, was published in the early 1970s. The targeted use of low carbohydrate dieting for blood glucose control in diabetics was not widely promoted until the 1980s, and even today it is not adopted by mainstream diabetes doctors. To this I should add that, at least anecdotally and from living in an area where diabetes is an epidemic (South Texas), those people who carefully control their blood sugars after type 2 diabetes diagnoses, in many cases with the help of drugs, seem to see marked and sustained health improvements.
Finally, an interesting implication of this study is that glucose intolerance, as defined in the article, would probably not do much to change an outside observer’s perception of a long-living population. That is, if you take a population whose individuals are predisposed to live long lives, with many naturally becoming centenarians, they will likely still be living long lives even if glucose intolerance is rampant. Without carefully conducted glucose tolerance tests, an outside observer may conclude that a damaging diet is actually healthy by still finding many long-living individuals in a population consuming that diet.
Quite a range, eh!? This covers the high end of normoglycemia, as well as pre- to full-blown type 2 diabetes.
In this investigation, called the Whitehall Study, 18,403 nonindustrial London-based male civil servants aged 40 to 64 years were examined between September 1967 and January 1970. These folks were then followed for over 30 years, based on the National Health Service Central Registry; essentially to find out whether they had died, and of what. During this period, there were 11,426 deaths from all causes; with 5,497 due to cardiovascular disease (48.1%) and 3,240 due to cancer (28.4%).
The graph below shows the age-adjusted survival rates against time after diagnosis. Presumably the N values refer to the individuals in the glucose intolerant (GI) and type 2 diabetic (T2DM) groups that were alive at the end of the monitoring period. This does not apply to the normoglycemic N value; this value seems to refer to the number of normoglycemic folks alive after the divergence point (5-10 years from diagnosis).
Note by the authors: “Survival by baseline glucose tolerance status diverged after 5-10 years of follow-up. Median survival differed by 4 years between the normoglycemic and glucose intolerant groups and was 10 years less in the diabetic compared with the glucose intolerant group.”
That is, it took between 5 and 10 years of high blood glucose levels for any effect on mortality to be noticed. One would expect at least some of the diagnosed folks to have done something about their blood glucose levels; a confounder that was not properly controlled for in this study, as far as I can tell. The glucose intolerant folks ended up living 4 years less than the normoglycemics, and 10 years more than the diabetics.
One implication of this article is that perhaps you should not worry too much if you experience a temporary increase in blood glucose levels due to compensatory adaptation to healthy changes in diet and lifestyle, such as elevated growth hormone levels. It seems unlikely that such temporary increase in blood glucose levels, even if lasting as much as 1 year, will lead to permanent damage to cells involved in glucose metabolism like the beta cells in the pancreas.
Another implication is that being diagnosed as pre-diabetic or diabetic is not a death sentence, as some people seem to take such diagnoses at first. Many of the folks in this study who decided to do something about their health following an adverse diagnosis probably followed the traditional advice for the treatment of pre-diabetes and diabetes, which likely made their health worse. (See Jeff O’Connell’s book Sugar Nation for a detailed discussion of what that advice entails.) And still, not everyone progressed from pre-diabetes to full-blow diabetes. Probably fewer refined foods available helped, but this does not fully explain the lack of progression to full-blow diabetes.
It is important to note that this study was conducted in the late 1960s. Biosynthetic insulin was developed in the 1970s using recombinant DNA techniques, and was thus largely unavailable to the participants of this study. Other treatment options were also largely unavailable. Arguably the most influential book on low carbohydrate dieting, by Dr. Atkins, was published in the early 1970s. The targeted use of low carbohydrate dieting for blood glucose control in diabetics was not widely promoted until the 1980s, and even today it is not adopted by mainstream diabetes doctors. To this I should add that, at least anecdotally and from living in an area where diabetes is an epidemic (South Texas), those people who carefully control their blood sugars after type 2 diabetes diagnoses, in many cases with the help of drugs, seem to see marked and sustained health improvements.
Finally, an interesting implication of this study is that glucose intolerance, as defined in the article, would probably not do much to change an outside observer’s perception of a long-living population. That is, if you take a population whose individuals are predisposed to live long lives, with many naturally becoming centenarians, they will likely still be living long lives even if glucose intolerance is rampant. Without carefully conducted glucose tolerance tests, an outside observer may conclude that a damaging diet is actually healthy by still finding many long-living individuals in a population consuming that diet.